20th October 2023

The UK’s former Prime Minister, Rishi Sunak, announced a policy in his 2023 conference speech to progressively increase the age at which people would be able to buy smoked tobacco products in England by one year, each year.
As an organisation that advocates for the responsible regulation of drug markets, this unconventional sales ‘ban’ demands our consideration. Getting to grips with whether the policy is justified and proportionate boils down to balancing the answers from a series of questions.
- Firstly, how serious is the problem the policy is seeking to address?
- Secondly, how serious is the imposition of the policy on personal rights/freedoms?
- Thirdly, will it work?
- And finally, are there preferable alternative ways of achieving the policy goal?
As detailed in the policy paper accompanying the announcement, the proposed change will:
“Make it an offence to sell tobacco products to anyone born on or after 1 January 2009. In effect, the law will stop children turning 14 or younger this year from ever legally being sold tobacco products - raising the smoking age by a year each year until it applies to the whole population”, the stated aim being to “ensure children and young people do not become addicted in the first place.”
The Government additionally notes that “As is the case with current age of sale legislation, the emphasis will be on those who sell tobacco products - the Government has never and will not criminalise smoking.”
It is a high profile and striking announcement, having few, if any conceptual or legal precedents in UK policy and law - only New Zealand/Aotearoa have implemented a similar rising age-based sales ban (in 2022), which was subsequently been abandoned by the incoming Luxon/National Party government. But it is now government policy for England, subject to a Commons vote on April16th 2023. Since the Labour party have already announced they will support it, it seems highly likely it will become law soon. (Note: the law technically will only apply to England as health policy is a devolved matter in Scotland, Wales and Northern Ireland. The UK Government states, however, that it "is committed to working closely with the devolved administrations as we develop these proposals, with a view to aligning policy approaches wherever this would improve outcomes" . Our understanding, subject to confirmation, is that the devolved Government's have agreed to implement it).
How serious is the problem the policy is seeking to address?
The public health burden of tobacco smoking in the UK is undoubtedly appalling, eclipsing, by a huge margin, all other legal and illegal drug health harms combined. The recent Khan review (discussed below) lays out some sobering statistics:
Almost 6 million people still smoke in England (this is more than the entire population of New Zealand)
Smoking is the leading cause of preventable illness and death in England; there were 75,000 GP appointments a month, more than half a million hospital admissions in total, and 64,000 deaths attributed to smoking in 2019 (for comparison there were 7,500 alcohol specific deaths, or 21,000 alcohol related deaths, in England in 2021, and 3060 deaths related to ‘the use’ of illegal drugs in 2021 in England & Wales)
When used as recommended by the manufacturer, 2 out of 3 smokers will die from smoking unless they quit
In 2019, a quarter of deaths from all cancers were connected to smoking
Around one third of adult tobacco consumption is by people with a current mental health condition, with smoking rates more than double that of the general population. These people die 10 to 20 years earlier, and the biggest factor in this is smoking
The annual cost to society of smoking in England is around £17 billion, with the cost to the NHS alone at about £2.4 billion – this dwarfs the £10 billion of income from taxes on tobacco products
3 in 5 of all households containing smokers living in poverty are in the North and Midlands, while fewer than 1 in 5 are in London and the South East
Perhaps because of the cultural ubiquity of smoking, or the fact that smoking related deaths relate to chronic long-term illness, which lacks the media shock factor of acute overdose drug deaths, we have seemingly become inured to the horrifying scale of smoking related health harms, and their deeply iniquitous impacts on the poor, marginalised and vulnerable.
How serious is the imposition of the policy on personal rights/freedoms?
The policy will be objectively discriminatory between groups of adults, purely on the basis of age, in terms of their ability to access a particular legal product market. This isn't the more easily justified distinction between a child and an adult but an entirely arbitrary line drawn between adults born before and after a given date. This will create the somewhat bizarre and unprecedented scenario of - in say, 20 years time - someone aged 35 being able to legally buy tobacco (on providing ID), but someone aged 34 being unable to do so.
The Equality Act 2010 includes provisions that ban age discrimination against adults in the provision of services and public functions. It is currently unlawful to discriminate on the basis of age unless there is an "objective justification".
Rights and liberties are, however, not absolute; they can be legitimately circumscribed in certain scenarios. Public health emergencies are a well understood case in point (most recently, for example, restrictions on movement and assembly during the covid pandemic). The bar for implementing such restrictions - and the infringements on liberties they incur - is rightly set very high. It should be even more so in this case given the restrictions are being imposed in such an arbitrary fashion. The question to evaluate then is whether that bar has been met; is the proposed objective justification sufficient?
There are some points to consider when evaluating the seriousness of any negative impacts on liberties resulting from this proposal. The first is the argument made by the PM in his speech that the ban would not impact current smokers, only people who had never smoked. The aim being to prevent people initiating use of risky smoked products in the first place.
The second is that the ban is on sales/purchase only, not possession and use. This is very different from the prohibitions on possession of illegal drugs like cannabis or cocaine under the Misuse of Drugs Act. Mere possession of these drugs can incur serious criminal penalties including life-long criminal records and prison sentences of up to 7 years, and life in prison for supply. This key difference immediately reduces the potential seriousness of impacts of such a sales ban relative to other drug prohibitions with which it has already been wrongly equated by some commentators. No one will get any form of sanction, let alone a criminal record or prison sentence, for cigarette possession, use, purchase or attempted purchase. Although not entirely clear from the policy paper, it appears that sales to an underage adult (i.e. an over 18 adult born after Jan 1st 2009) will also be an administrative or civil offence (subject to fines), not a criminal or imprisonable one.
Someone born after Jan 1st 2009 would, therefore, still be allowed to legally possess and smoke cigarettes, just not able to personally buy them in England. So unless other restrictions were also introduced, such adults could still smoke cigarettes shared by others, or buy cigarettes in another jurisdiction (for example, in a devolved UK region that has not implemented the policy, or in duty free at an airport before heading home from a holiday). ‘Proxy purchase’ (i.e. someone over the age threshold to buying cigarettes for someone under it) will also be an offence (sanction to be determined), as it already is (since 2014), regards buying for people under 18. Inclusion of this additional proxy purchase offence would in practice be largely symbolic, as it would be near impossible to meaningfully enforce for adults supplying each other.
The third point is that the sales ban will only apply to tobacco products. It is not a wider form of nicotine prohibition; other nicotine products will still be available to all UK adults, significantly including vapes (Electronic nicotine delivery systems, or ENDS), oral nicotine pouches, and various forms of nicotine replacement therapy (patches, gum etc).
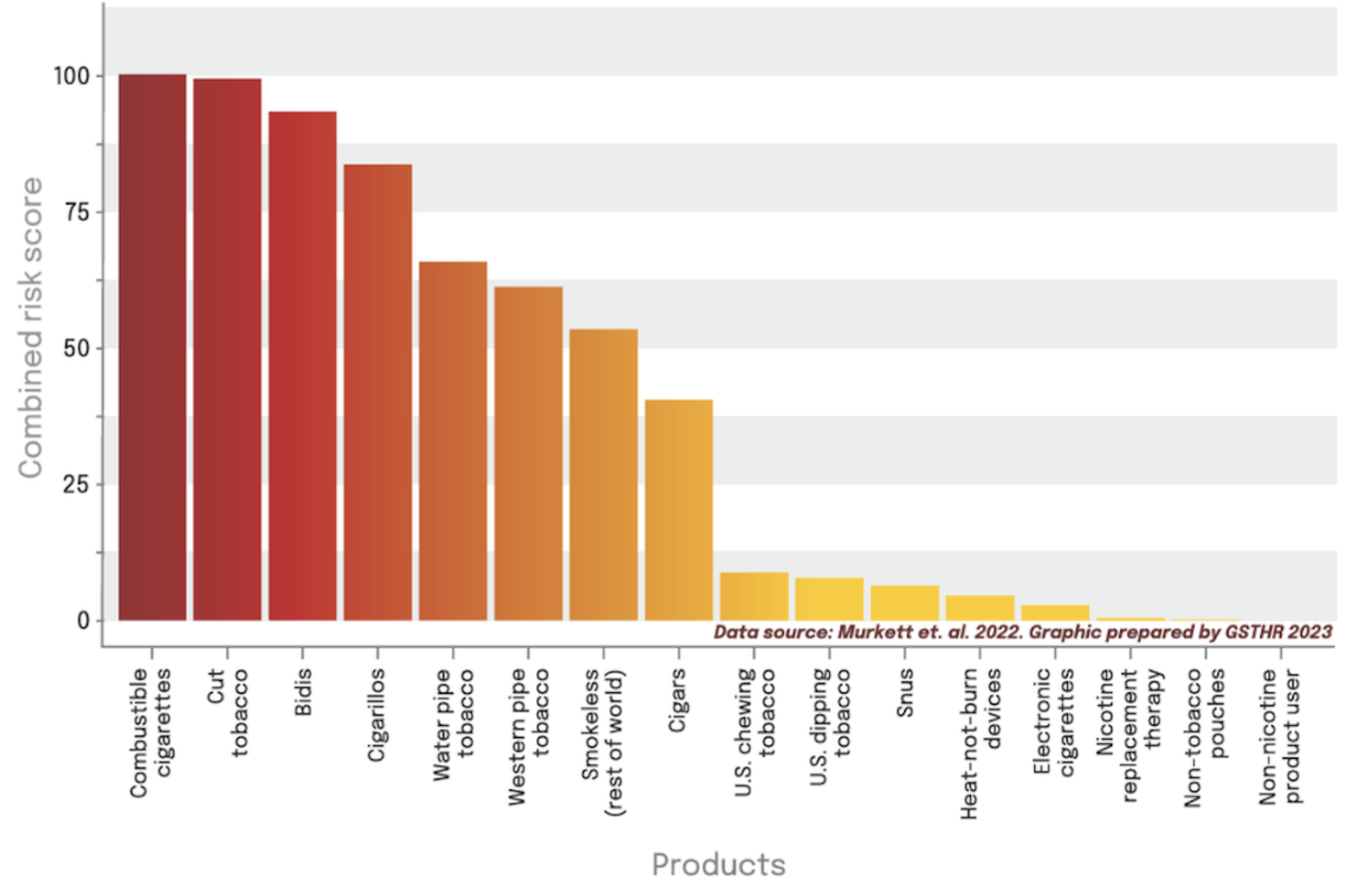
The scope of the controls, even if well-intentioned, is unfortunately misaligned, with the Government drawing a politically informed boundary between tobacco and non-tobacco products, rather than a risk-informed boundary between combustible/non combustible products. The result of this misalignment (seemingly shaped by more strident voices from the old school tobacco-control community) is that sales of non-smoked tobacco products (including snus and heat-not-burn tobacco devices) which can, like vapes, serve as useful forms of harm reduction, will also be banned for sale alongside cigarettes. It is hoped that this ill-considered and counterproductive move will be revisited during the pre-legislative scrutiny period.
Putting aside this inescapably daft shortcoming, the proposed ban will most significantly impact sales of cigarettes and smoked tobacco which are, by far, the most dangerous nicotine products (see graph below). It is reasonable when evaluating the impact on individual rights, to make the distinction between a wider nicotine product sales ban, and the ban on one particularly risky form of smoked/combustible tobacco product that contains nicotine. Indeed it is clear that the discussion on smoked tobacco controls cannot take place independently of considerations around the wider nicotine market, a point made clear in the Government’s new policy discussion paper and its emphasis on encouraging people to swap from smoking to vaping. Any kind of ban on any smoked tobacco product sales - age based or otherwise - becomes much harder to justify in the absence of access to safer alternative nicotine products, specifically including vapes/e-cigarettes/ENDS, and oral nicotine pouches/snus.
The worst case scenario is where smoked tobacco is actively preferenced in legal markets over vastly safer non combustible products, either by heavy restrictions or complete bans on the latter product categories. Regrettably, this is exactly what has happened in India, where bidis and cigarettes remain widely available, alongside a comprehensive ban on vapes, and in Australia, where cigarettes remain widely available, but vapes are available on prescription only as medical products. Notably, since Australia’s ill-considered move in 2021, their progress in reducing smoking has stalled (rates have in fact risen marginally) relative to other countries with more pragmatic policies on vapes. In this context, it is deeply concerning to hear Mark Drakeford, first Minister of Wales, expressing support for the Australian policy.
There are, of course, important policy debates relating to the responsible regulation of vapes and other non smoked nicotine products; particularly around disposable vapes and sustainability, licensing and enforcement of vendors, product safety, and controls on product marketing, flavourings, price and availability (with adolescent access and use highlighted as a key concern). These issues were also briefly noted in the PMs speech, and a public consultation on proposed new vape controls has been launched as a separate element of the new smoke-free policy.
Will it work?
A key factor in evaluating the proposal’s merits and justification must inevitably be one of efficacy: Will it actually work? Even if one accepts the case that there is a public health emergency of a scale sufficient to warrant such an illiberal legal imposition, this is still only sustainable if, a) the policy delivers on its objectives, and, b) there are not alternative policy approaches that could achieve the same goals without the potential costs and arbitrary impacts on rights implicit in the age-based ban.
Since the policy has so far only been implemented in New Zealand, and only very recently, we do not have any real world evidence yet. New Zealand has, however, estimated that, if well-enforced, prohibiting the sale of tobacco to anyone born after 2009 could reduce their smoking rates to half of current rates within 10 to 15 years. Similar modelling from the the UK DHSC "forecasts that this measure [under various scenarios and in conjunction with other proposed interventions] could further reduce smoking rates in England among 14 to 30 year olds such that, within 3 to 10 years of implementation, they could be half of current rates and close to 0% as early as 2040." This modelling is ‘provisional’ and will only be published in the upcoming Impact Assessment - so is not possible to scrutinise at this point.
There is also - as mentioned in the PM's speech - compelling evidence from the UK, that when the age of cigarette purchase was increased from 16 to 18 in the UK this led to a 30% fall in prevalence in that age group. Similarly, in the US, when the legal age of access to cigarette sales was increased from 18 to 21, there was a 39% fall in that age group.
It was estimated in 2017 that each year around 207,000 children in the UK start smoking, and although this number will already be lower due to smoking/vaping trends, the number remains non-trivial. Among adult smokers, about two-thirds report that they took up smoking before the age of 18 and a remarkable 83% before the age of 20. The rising age policy would initially only impact those who would have started after 18 - with only indirect impacts on under 18s thereafter, presumably via reduced access to peer/sibling supply and changes in youth smoking culture more generally.
Central to the concept of rule of law is a requirement that laws are both clearly understood and enforceable, and questions have inevitably been raised, not least by retailers, about the practicality of enforcing the proposed sales ban, with its unprecedented ever-shifting ID-mandated age-access threshold. It will be possible - but it will also be difficult, frustrating and messy.
It is also reasonable to expect that the intrinsically arbitrary nature of the proposed rising age cutoff will not command the same public support and levels of compliance of more familiar adult/non-adult access restrictions. While polling suggests there is general public support for tougher smoking controls, we haven’t yet seen polling on the rising age sales ban specifically (although one suspects the Government will have road tested it in focus groups, and they also floated the idea a few weeks before the official announcement to see how it would be received). Majority public support for tougher controls does not inevitably translate to support amongst the shrinking minority of smokers themselves, who are likely to be more resistant. In this case, however, we have the unusual scenario of a new tobacco control measure that doesn’t directly impact current smokers, many of whom want to quit and support the idea of reducing youth smoking as well. The policy will only impact people currently aged 14 or below, giving the Government a 3-4 year cushion before any of those born after the cutoff date reach 18, and the impact of restrictions even start to be felt.
The extent to which the age based sales restrictions will be ignored, or evaded by diversion and unlicensed sales (and potential harms of a parallel illegal/quasi-legal market) therefore remains to be seen. Impacts of previous restrictions being introduced suggest it is likely to fuel some degree of displacement to illegal supply and informal markets, alongside any impacts on reduced prevalence. But in this case, any such effects will only emerge slowly as the age restrictions bite over an extended period, and these negative impacts will be mitigated by the ongoing contraction in market demand more broadly.
Are there alternative approaches that could achieve the same goal?
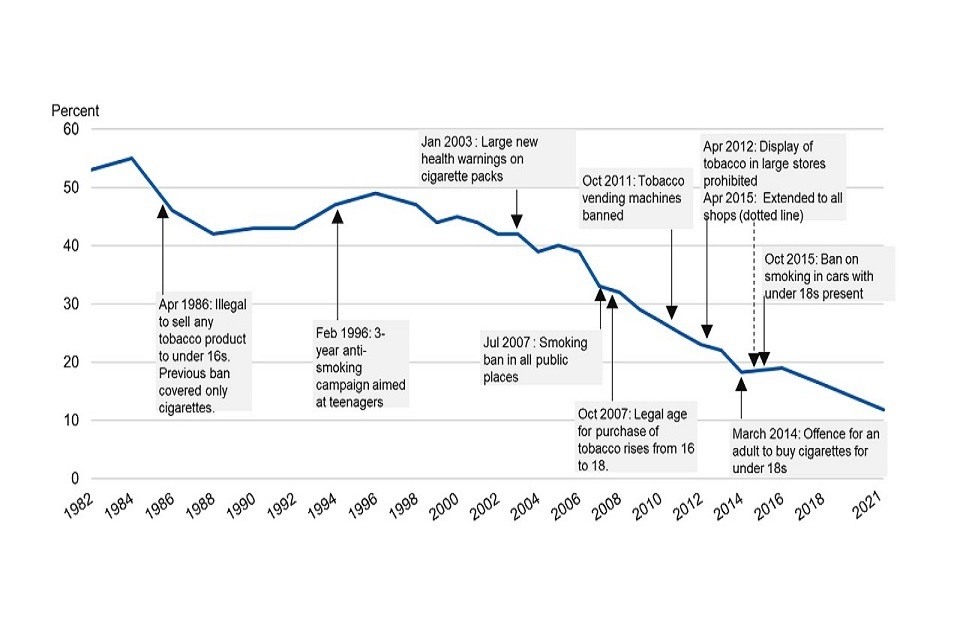
Stricter regulation of cigarette sales and use, combined with meaningful investment in public health and risk education and cessation services, has driven a long term reduction in smoking prevalence over the last 5 decades in the UK - from over 45% in 1974 to around 12% today. The ratification of the WHO framework Convention on Tobacco Control in 2004 has been a key moment in this process. This can be seen as a legitimate modern public health success story. Tobacco control, especially in the context of rising use and health harms associated with unregulated illegal drugs over the same time span, is one key aspect of drug policy where the UK has not been shockingly poor by global standards (significantly because it has been approached primarily as a public health challenge led by health agencies, rather than an enforcement challenge led by the Home Office).
During this period, regulatory interventions have included; progressive increases in taxes, a complete advertising ban in 2003, a ban on smoking in public spaces in 2007, raising age of purchase from 16 to 18 in 2007, a ban on tobacco vending machines in 2010, a ban on point of sale product displays in 2012, and the introduction of plain packaging in 2017. In addition to these regulatory interventions the emergence of nicotine vaping products around 2012, essentially a disruptive technology with welcome, if largely accidental, health benefits helped accelerate the fall in smoking since that time as growing numbers of smokers switch, or younger people adopt vaping instead of smoking.
Given the extent of regulatory interventions and controls already in place, there is evidently a shrinking menu of more conventional options left, with gains increasingly marginal. That said, the argument has reasonably been made that given the scale of smoking public health harms, even marginal gains translate into major wins at a population level. A 1% fall in smoking, for example, translating into many 1000s of smoking related deaths avoided annually in the longer term.
In 2019 the Government published a green paper on ‘Advancing our health: prevention in the 2020s’ which included "an ambition for England to become ‘smokefree’ by 2030 – achieved when adult smoking prevalence falls to 5% or less". Last year an Independent review by Dr Javed Khan into this 2030 ‘smokefree’ ambition concluded that the 2030 goal was likely to be missed under the current regime by at least 7 years. Khan does, however, make a series of suggestions for how it might be delivered on time. These included the rising age threshold proposal announced last week, but notably also:
Increased funding for education and cessation services. Khan notes that ‘Over the last decade, smoking interventions have been skinned to the bone by reductions in funding. This decline must be reversed. Local stop smoking services provide a highly cost-effective approach to help people quit smoking since 2016, local authority spending for these services has declined by 40% (in real terms) compared to a 21% decline for the public health grant overall. Additionally, budgets for marketing campaigns to encourage smokers to quit have dropped from £23 million to £2 million in 10 years’
Promoting vaping, Khan recommends ‘The government must embrace the promotion of vaping as an effective tool to help people to quit smoking tobacco. We know vapes are not a 'silver bullet' nor are they totally risk free, but the alternative is far worse.’ additionally calling on government ‘to accelerate the path to prescribed vapes and provide free Swap to Stop packs in deprived communities’
Khan credibly argues that no one intervention is a ‘silver bullet’, and that the age based sales ban should be seen as part of a package of measures that collectively are needed to achieve the smokefree target. So far the Government has - it must be acknowledged; commendably - largely followed through on Khan’s key recommendations, initiating the swap to stop programme promoting vaping as a cessation aid, increasing funding for cessation services by Khan’s recommended £70 million, as well as some other initiatives targeting vulnerable populations such as offering financial incentives to pregnant women to stop smoking. The rising age based sales ban is one of the final parts of the Khan review recommendations still to be implemented.
Potentially some of these things could be done better, or faster. Building on existing controls, prices could potentially be made a bit higher, sales could be restricted to specialist licensed outlets (although again, potentially incentivising diversion/smuggling), and cigarettes could be made a bit more unattractive (there is a proposal for health information insets to be included in every pack, while in Canada health warnings are being printed on individual cigarettes). A case could certainly be made for ditching the rising age-based sales ban if this basket of other measures was implemented. But the counter argument is that this is not an either/or; they all have an impact (even if size of impacts is uncertain), and - given the scale of the public health emergency - we should be doing all of them, since, as noted, when the problem is this grave, even marginal falls in prevalence represent big public health wins.
Perhaps the most obvious alternative approach that hasn’t been proposed by the Government (or, more surprisingly, the Khan review) is a different kind of age access intervention. One, in fact, noted in the Prime Minister’s speech. That the US move to increase the purchase age from 18 to 21 was demonstrably effective does beg the question of why a similar move couldn’t work in the UK too. The obvious answer is that it would work, in all likelihood achieving similar outcomes in the same target youth populations, albeit much quicker, since it would take effect immediately. It would also be more practical in its enforcement, and more legally consistent by avoiding the peculiarities and arbitrary nature of a rising age sales ban. On the downside it would certainly have a bigger immediate negative impact in terms of fuelling diversion to parallel informal/criminal markets - but given their existing scale (around 16% of the cigarette/tobacco market) this is arguably a manageable burden. The problem for the Government is perhaps that such a move would feel more illiberal (even if objectively it isn’t), with an existing right of purchase being removed for those currently in the 18-21 age group. This would, in turn, translate into a much higher degree of political opposition from a key voter demographic (with an election on the horizon), and leave this Government more exposed to the much feared accusations of nanny-statism etc.
In summary
So returning to the original breakdown of the question to tease out if the move is justified and proportionate; Is the problem serious enough to warrant further Government action? - clearly yes, the status quo remains unacceptably grim and progress is too slow. But, proposed interventions need to be justified on a case by case basis, so…
How serious an infringement on rights and liberties is the age based sales ban? While objectively discriminatory and illiberal, its novelty and unfamiliarity perhaps makes it harder to form a view. It is, however, not a new form of criminalisation or a prohibition in the classic sense, and the continued availability of other nicotine products, including vapes and nicotine pouches, is important context (the ill-considered inclusion in the ban of non-smoked tobacco products notwithstanding). Continuing the progressive ratcheting up of restrictions on the most risky forms of nicotine products, while making safer products relatively more available, could be argued to be more a form of responsible nicotine regulation, than prohibition.
Will it work? Probably - It is reasonable to assume it will, over an extended period, have a meaningful impact on initiation and young adult prevalence and related smoking health harms - although impossible to estimate with much precision.
Are there alternative approaches that could achieve the same goal? While the number of available remaining options for increased tobacco controls is narrowing, there is more that could be done. But many of these things are happening even if there are some that are yet to be adopted or that could be done better and faster. Khan reasonably argues that these are not alternative interventions to the age based sales ban, but part of a package that needs to include all of them. The failure to explore raising tobacco product purchase age to 21 as a credible alternative - given its proven efficacy in the US - is the most obvious missing alternative (as opposed to additive) control.
A view on whether the rising age sales ban is justified will therefore come down to a judgement of how obnoxious one finds the arbitrary/discriminatory nature of its implementation in principle, and whether one views its certain (but probably, in practice, marginal) costs as outweighing the less certain, but likely meaningful public health benefits, given the slim menu of politically palatable alternatives.
Of course, whatever your view - it is likely happening in England regardless, and that will influence the debate globally. Indeed, other countries are already contemplating the policy, including Australia (although they will urgently need to revisit their vape ban if they do), and it also seems likely that the devolved UK regions will have to make a call on this soon.


