16th June 2023

New analysis from David Mansfield, the leading expert in the field, suggests that the ban on opium threatened last year by the Taliban has come to pass, and there is an estimated 80%+ reduction in Afghan opium production - which supplies some 95% of the European heroin market.
What are the implications of this opium ban for Afghanistan and the region; for global opium and heroin production, and for UK policy?
We outline three possible scenarios that could come out of recent developments in Afghanistan and put forward proposals for preparedness and risk mitigation.
Scenario 1: Opium ban is not sustained
Scenario 2: Opium ban is sustained, production is displaced to other regions
Scenario 3: Opium ban is sustained, displaced production does not meet demand, and synthetic opioids (and other drugs) fill the market void
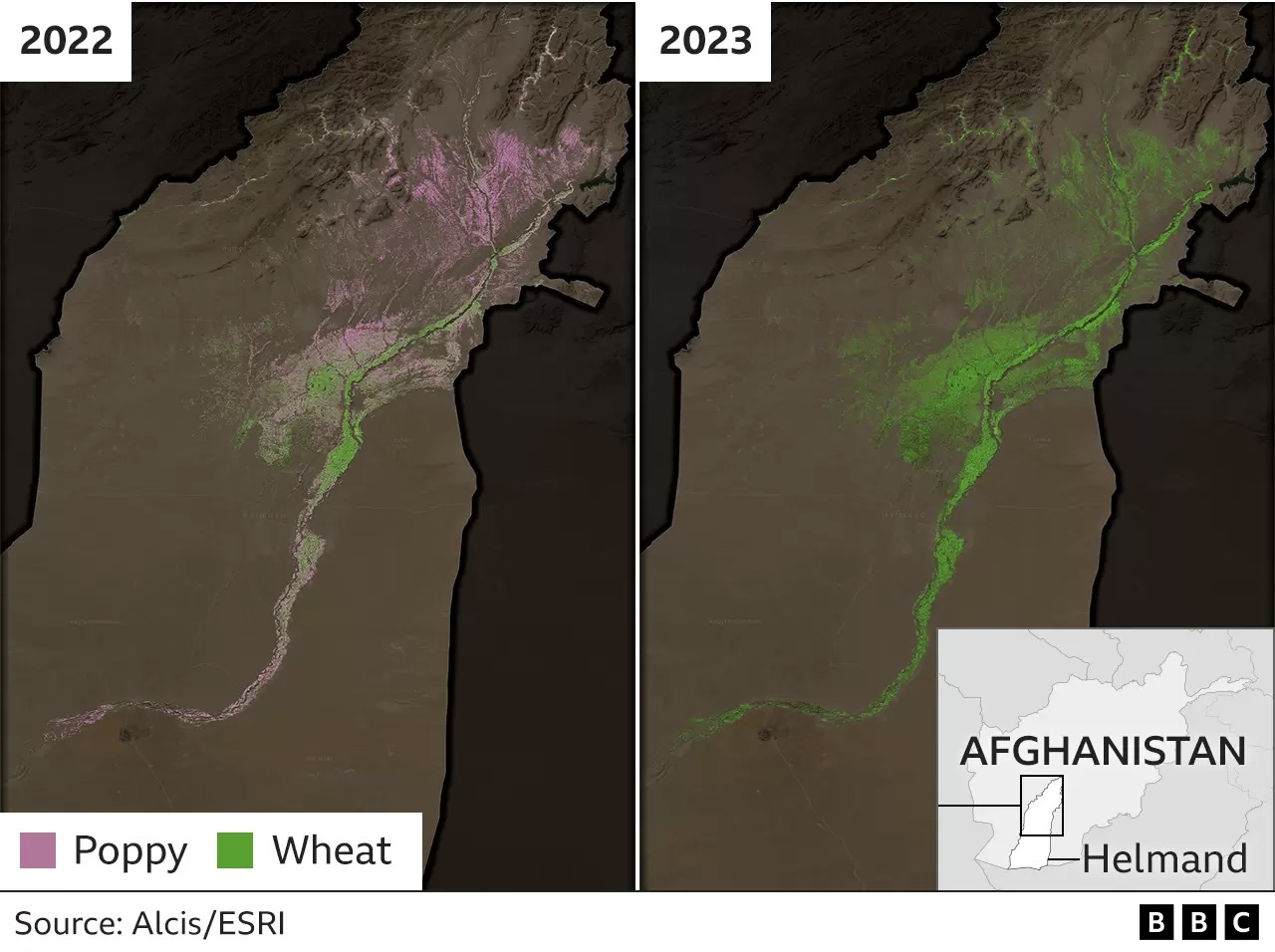
"The high resolution imagery of Helmand province shows that poppy cultivation is down to less than 1,000 hectares when it was 129,000 hectares the previous year," according to David Mansfield, a reduction of over 99%. The current opium ban is seeing; “truly unprecedented reductions in poppy cultivation… a reduction in this one province alone that surpasses any prior national poppy ban in Afghanistan”.

Scenario 1: Opium ban is not sustained
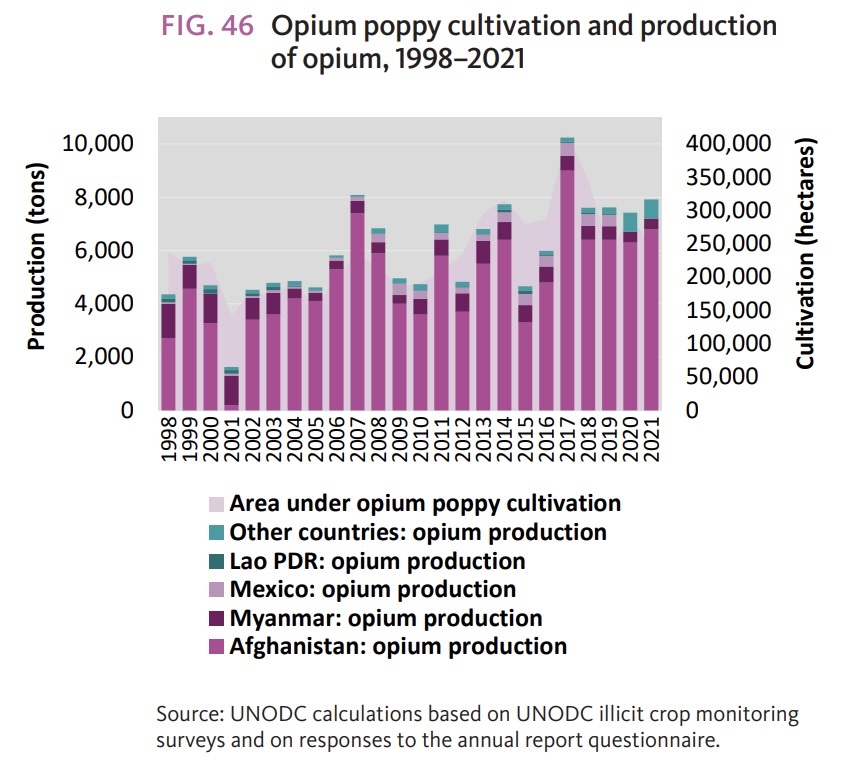
A previous Taliban opium ban in 2000-1 that was not sustained after Taliban control ended following the Allied occupation of Afghanistan, provides a precedent that can inform scenario planning. It similarly reduced opium production to low levels (see graph below from the UNODC World Drug Report 2022). However, stockpiles from previous bumper harvests meant that while opium prices rose dramatically in Afghanistan, the net flow of heroin into European markets was largely uninterrupted.
The price of opium only constitutes a small fraction of the street-level price of heroin in the West. Indeed the ban on opium growing, which was seen by many as an attempt to strengthen relationships with Western aid donors, may have only served as a price support mechanism. By boosting the price of opium stocks sold in lieu of new production the ban may ultimately have profited the Taliban, who derive a substantial income from informal taxes on the opium trade.
In this context it is difficult to know whether the ban is going to be enforced in the long term by the Taliban, who publicly make both a public health and moral/religious case for its imposition, or whether it is more of a short-term political strategy to appease the international community and potential donors.
On the ground in Afghanistan there is also the very real prospect, indeed emerging reality, of the country's opium farmers - many of whom are driven into illicit production as a form of economic survival - being plunged further into poverty. With few economically viable options, opium offers a far more reliable source of income than less hardy, and less profitable conventional crops such as wheat.
So the first scenario is that the ban will not be sustained for multiple growing seasons, with the Taliban ultimately opting not to risk one of its dwindling sources of income (especially in the event of international aid not being forthcoming), and potential hostility from significant swathes of the population further driven into poverty. Like the 2000/01 ban, current opium stockpiles may prevent any substantial impact on net heroin production and supply in major Western markets in the short term.
Scenario 2: Opium ban is sustained, production is displaced to other regions
A second scenario is that the ban is effectively maintained at its current level and opium production from Afghanistan decreases by 80-90% in the medium- to long-term, even if there is some displacement of production to marginal regions of Afghanistan where the Taliban has weaker control. The 2023 planting season in November will be a crucial indication of this occurring, with rumours presently suggesting the ban will be imposed again this year.
The contraction of supply would likely increase opium prices further, especially as stockpiles are exhausted, incentivising new actors to enter the market. This could potentially mean: expanded production in traditional opium producing regions such as the golden triangle; increased diversion of licit opium production in major producers such as India and Turkey; or displacement of production into new regions in central Asia, South East Asia, or elsewhere. One of the attractions of opium is that it grows well in a wide range of climates. However, the sheer scale of new or diverted production needed to replace Afghan opium, set up laboratories to convert it to heroin, and increase capacity in trafficking routes from other areas would not happen overnight. Nor would building the confidence of farmers to commit their livelihoods to growing the crop in other countries.
Scenario 3: Opium ban is sustained, displaced production does not meet demand, and synthetic opioids (and other drugs) fill the market void
A third scenario is that the Afghan opium ban is sustained, opium production from elsewhere does not rise enough to counterbalance the impact, and the heroin supply is substantially reduced. According to David Mansfield, following the 2000/01 opium ban, it took 18 months before there was a significant drop in the quality of heroin in UK markets, and two years for average purity to fall from 55% to 34%. However, this suggests even a two year ban - given the current one appears more comprehensive - would likely have a significant effect, with rapidly rising impact after that.
In 2001 there was a ‘heroin drought’ in Australia which saw substantial reductions in heroin use, and related harms, and more people seeking treatment. But it also saw substantial increases in use of cocaine, amphetamines and to some extent benzodiazepines. However, the drugs market has changed since then. It is entirely plausible that ongoing demand for opioids in European (and other) markets could instead increasingly be met by production of illicit synthetic opioids, such as fentanyl, that were not readily available in 2001.
The potential for such a phenomenon has already been demonstrated in North America where illicit heroin use has been largely displaced by illicit fentanyl (and various fentanyl analogues) produced and supplied by Mexican cartels - mainly using precursor chemicals from China. Historically, Mexico has also been the source of much of the heroin used in the US.
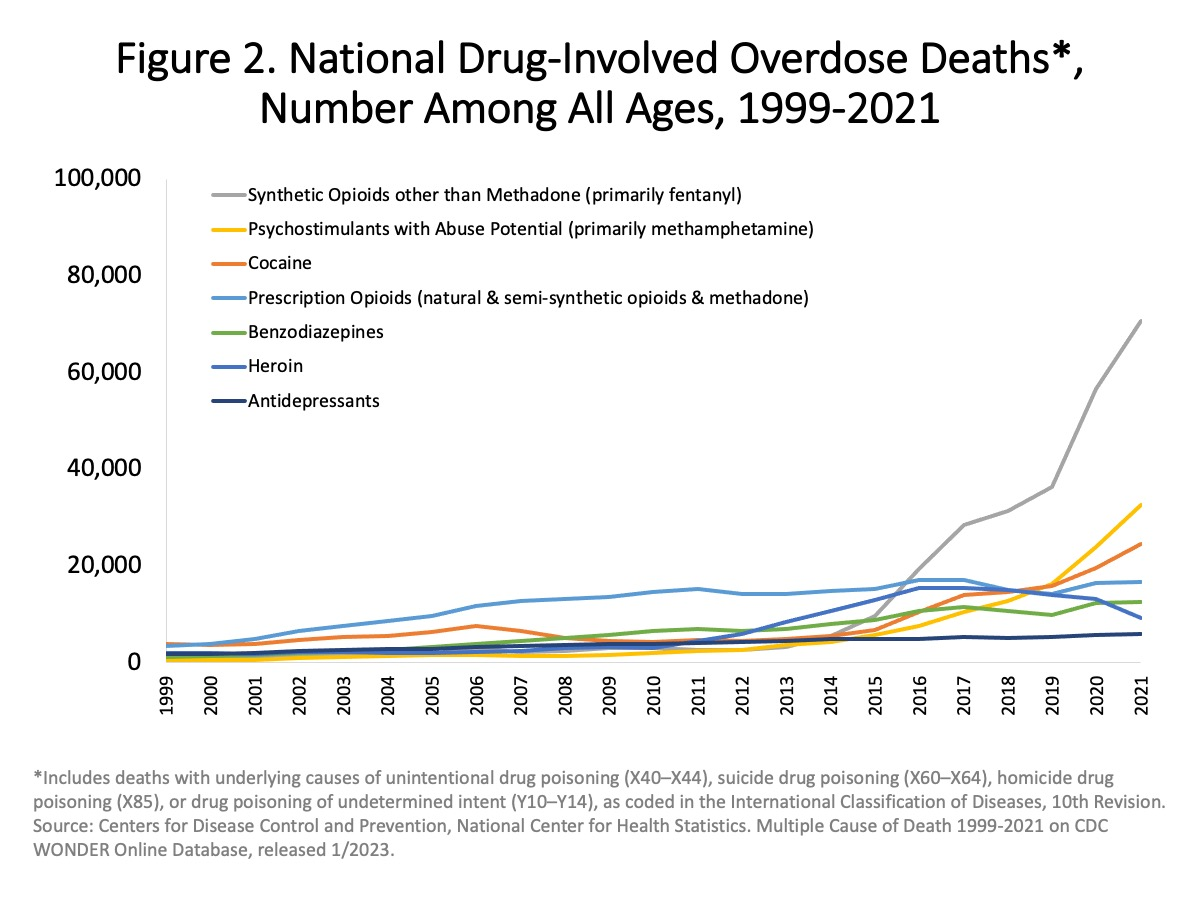
Fentanyl, relatively easily manufactured in illicit laboratories, is 50 times more potent than morphine (some analogues many times more potent still). This makes it an appealing prospect for entrepreneurial organised crime groups (OCGs): why traffic 50 kilos of heroin when you can traffic one kilo of fentanyl, potentially avoiding long trafficking routes, and instability of opium crops? But its potency also makes fentanyl a dramatically riskier drug, fuelling the terrifying spike in opioid related deaths witnessed in the US and Canada in recent years (see graph below). There has been much speculation about why fentanyl has not already penetrated European markets and replaced heroin to a greater extent. It may be that suppliers simply did not want to risk losing their customer base unnecessarily, or it may be down to some unknown interplay between regional OCGs. But whatever the reason, if there is very little heroin available, that dynamic, and the shape of the market will surely change.
Even if the drivers, and more precise contours of such a shift differ from the North American experience, the basic economic dynamics remain the same; OCGs do not respect drug laws, they live by the laws of supply and demand. While demand for opioids remains high, particularly among a small population of high-intensity long-term users, the profits on offer mean that criminal entrepreneurs will always seek out ways to exploit it. Online darknet sales of opioids could expand rapidly, there are likely to be increased pressures towards diverted prescription opioids, and Mexican cartels - with established production capacity and infrastructure for trafficking to Europe (for cocaine) - could jump on this new opportunity. EU based OCGs, already engaged in synthetic drug production, and controlling the heroin distribution networks could do the same.
Shocking as the spectre of further encroachment of fentanyl into UK illicit opioid supply chains may be - the landscape is already more troubling. Fentanyl is just the first of a new wave of synthetic opioids, notably including nitazenes - a family of compounds that include isotonitazene (some 40-50 times more potent than morphine). Nitozenes are already associated with 100s of deaths in the US, and with 24 fatalities in the UK in 2021. WEDINOS analysis in the UK shows nitazenes currently appearing in a range of substances sold as heroin, diazepam, oxycodone, oxycontin, xanax, alprazolam and even cannabis and THC vape liquid. There is also growing concern about the use of illegal benzodiazepines - implicated in hundreds of drug-related deaths in Scotland (often when used with heroin) every year, and growing numbers across the UK and some other countries. Again, if heroin becomes less available, the incentive to use ‘street benzos’ as well will increase.
Perhaps the most likely scenario is that there will be elements of all of the three scenarios above. The opium ban is maintained at first with significant impacts, but as time passes it will not be as strictly enforced, with Afghan opium production returning - but at a much reduced level; some demand is met by production displaced to other regions, but the shortfall is met by increased illicit synthetics. However, even if the opium ban were lifted in future years and heroin production is resumed, the N.American experience suggests it is likely to be impossible to put the fentanyl/other drugs genie back in the bottle.
How the UK must prepare to mitigate risk
There is a huge risk of increased drug overdose deaths involved if the heroin supply does dry up, and a switch to synthetics occurs. The UK and other countries who are in a similar position must urgently begin contingency planning and delivery of interventions.
Led by all the Governments in the UK (Westminster, Holyrood, Senedd and Stormont), this should be happening at the national, regional and local level, pulling together local authorities, public health, treatment groups, police and the NHS among others.
Decades of failure demonstrate there is no supply-side enforcement solution - it would only make things worse. Instead we need learning from successes and failings in Europe and North America to deliver a truly public health and harm reduction led approach. A failure to do so could be catastrophic. The UK’s already record high drug-related death rates could rise much further.
Planning must include fast track expansion or delivery of:
- Enhanced and innovative harm reduction interventions that have a strong evidence base to engage key target groups, reduce overdose risk, or treat overdoses. These include:
Expansion of Police Drug Offence Diversion Schemes so those caught with drugs for their own use (or minor supply offences) are given drug harm reduction education, treatment and support services, rather than arrest or prosecution.
Provide treatment and other services with Fentanyl testing strips for clients to use on their drugs.
Expand overdose training and carrying of Naloxone by police and other services, and provision to people who use drugs, their associates, and others who live or work in higher overdose risk areas.
Increase surveillance including Expanding Drug Alert Early Warning Systems, combining information from a range of sources including city centre drug checking services, drugs obtained for alert systems, border force, police and services.
Guidance and coordination for housing services including encouraging more hostels to allow residents to inform staff when they are going to use drugs so overdoses can be treated, rather than using secretly or in the street.
Ensure hospitals promptly treat withdrawal, avoiding discharges against medical advice, and that opioid agonist therapy (OAT) is promptly restarted following discharge (a significant proportion of overdoses are shortly after leaving hospital)
Ensuring coordination with prisons to continue OAT on both admission and release.
See a Public-health Approach to Drugs for a template set of policies Transform developed with experts in the public health and treatment field, that we believe should be implemented to reduce harm whether there is a heroin drought or not.


