15th November 2018

The central aim of Swedish drug policy is to create a drug-free society. To achieve this aim, the country has adopted a punitive, enforcement-led approach to drugs. It is this approach, some have argued, that is responsible for Sweden’s historically low levels of drug use. This apparent success of the Swedish model is therefore often presented as an argument against drug policy reforms such as decriminalisation and legal regulation.
However, the degree to which Sweden’s low prevalence of drug use can be attributed to its repressive approach is highly questionable, as research consistently shows that wider social, economic and cultural factors are the key drivers of drug prevalence – not the harshness of enforcement.
Also of note is that levels of drug use in Sweden, while in relative terms still very low, are increasing. Furthermore, the Swedish model – in particular its antipathy to proven harm reduction measures – has had serious negative consequences that are almost never mentioned by its advocates. These include alarmingly high rates of hepatitis C among people who inject drugs, and a 600% increase in drug-induced deaths over the last 20 years.
Background
In its attempts to achieve a drug-free society, Sweden has pursued a ‘zero-tolerance’ approach to drug use, investing heavily in law enforcement, prevention, and abstinence-based treatment. This policy model emerged in the 1960s, following the rise in drug use that was observed across much of the developed world at that time. Since then, the maximum penalties for drug offences have been gradually ratcheted up, and in 1988 Sweden took the unusual step of criminalising not only drug possession, but drug use too.
Initially, use was only punishable by a fine, but this changed in 1993, when imprisonment was included as a potential sanction. The introduction of this harsher penalty was a prerequisite for police to be able to conduct blood or urine tests without individuals’ consent.1 30,000 such tests now take place annually, on top of the 10,000 to which drivers are subjected.2
The number of people convicted of drug offences has more than doubled over the last 10 years. And while fines are by far the most common penalty issued, the vast majority of convictions (83%) are for simple drug possession or use.3 It is therefore minor offenders who are overwhelmingly criminalised.
Drug Use
In 2007, the UN Office on Drugs and Crime produced a report entitled ‘Sweden’s successful drug policy: a review of the evidence’.4 5 In the introduction, UNODC director Antonio Maria Costa boldly stated: ‘societies have the drug problem that they deserve’, noting specifically that ‘in the case of Sweden, the clear association between a restrictive drug policy and low levels of drug use, is striking.’6 This narrative of Sweden as an example of effective prohibitionist drug policy has been widely repeated by opponents of reforms such as decriminalisation and legalisation.
However, studies have consistently failed to establish the existence of a link between the harshness of a country’s drug laws and its levels of drug use. A 2008 study using World Health Organization data from 17 countries (not including Sweden) found: ‘Globally, drug use is not distributed evenly and is not simply related to drug policy, since countries with stringent user-level illegal drug policies did not have lower levels of use than countries with liberal ones.’7 Many other large-scale studies – including most recently a study by the UK Home Office – have come to the same conclusion.8
Other facts further undermine the notion of a causal link between Sweden’s harsh drug law enforcement and its low levels of drug use:
- Although one of the main intentions behind criminalising drug use in 1993 was to deter young people from taking drugs,9 the lifetime use of any drug by 15-16-year-olds increased from 6% to 9% between 1995 and 201110
- While alcohol and tobacco use among young people is declining, illicit drug use is rising.Again, between 1995 and 2011, last-month cannabis use among 15-16-year-olds rose from 1% to 3%.11 The lifetime use of illicit drugs other than cannabis among this group has also increased, from 2% to 4%12
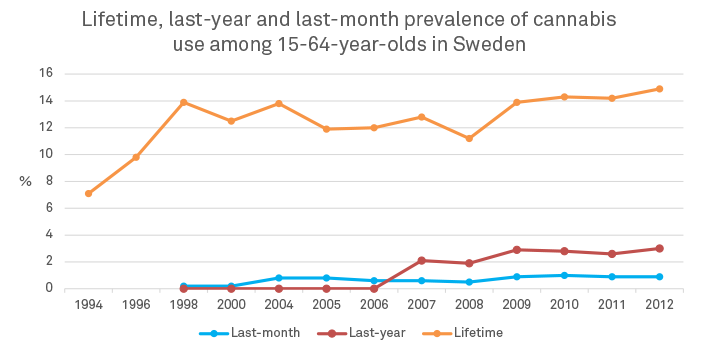
- Among the general population (15-64-year-olds), drug use is rising. By two out of three measures (last-year and lifetime) cannabis use is now higher in Sweden than in Portugal, which decriminalised the personal possession of all drugs in 200113
- The proportion of the adult population that have used amphetamines in their lifetime has risen from 1.4% in 1994 to 5% in 2008 (the latest year for which data are available)14
- The lifetime use of inhalants and non-prescription use of tranquillisers and sedatives among young people has risen from below the European average to above it15
- Countries that follow a similarly punitive approach to Sweden’s (such as the UK and France) have significantly higher levels of drug use
Research suggests that the prevalence of drug use is driven primarily by a complex interaction of social, economic and cultural factors. Drug policy – and specifically drug law enforcement – has, at best, a marginal impact. Furthermore, the prevalence of problematic drug use correlates closely with high levels of social deprivation and social inequality – two measures that Sweden has historically fared very well on, since it is a rich country with a highly developed and generous welfare state (although in recent years wealth and income equality has worsened in the country). Sweden also has a somewhat socially conservative and abstemious culture, with relatively low levels of alcohol and tobacco use, and low levels of prescription drug use too.
But it is important to recognise that the effectiveness of drug policy should not be judged on the prevalence of use alone; there are a number of other indicators of success, and on these, Sweden fares substantially worse.
Insufficient harm reduction
Sweden’s focus on achieving a drug-free society has created a hostile environment for interventions that seek to reduce the potential harms of drug use, rather than preventing or eliminating drug use itself.16 A major review published in 2011 recognised the need to scale up harm reduction,17 but the previous government failed to act on it because of its commitment to an abstinence-based approach. Campaigners hope that the new government will revisit the recommendations, but currently the provision of harm reduction services remains poor by European standards, and by those recommended by the World Health Organization and the UNODC:
- There are only five needle exchanges in the whole country – and none in Gothenburg, the second-largest city
- Opiate substitution treatment (OST) is available, but is subject to heavy restrictions (particularly for methadone)
- Some OST centres have a zero-tolerance stance on the use of other drugs, leading to fewer people being retained in treatment
- OST in prison started as a pilot project in 2007 and was continued as a national programme in 2010, but coverage remains poor18
- Sweden has no provision of safe injecting kits; no universal hepatitis B immunisation programme; limited availability of overdose information and overdose response training; and naloxone – which can counter the effects of opiate overdose – can only be obtained through medical personnel and is not available for take-home use19
- Sweden has no supervised drug consumption facilities (such as those seen in Denmark, Germany, the Netherlands, Spain and Norway), and collects no data on harm reduction provision in recreational settings such as night clubs and festivals

Hepatitis C
This lack of harm reduction services has led to some extremely negative outcomes. Rates of hepatitis C among injecting drug users in Sweden are some of the highest in Europe. Hepatitis C is a blood-borne virus that, left untreated, can lead to cirrhosis of the liver and death. The Stockholm needle exchange has recorded prevalence of the virus at 74% in 2013,20yet no official, national-level estimate is available, meaning it is unclear how many people need treatment for it, or how many people need access to needle and syringe programmes (NSPs).
Drug-induced deaths
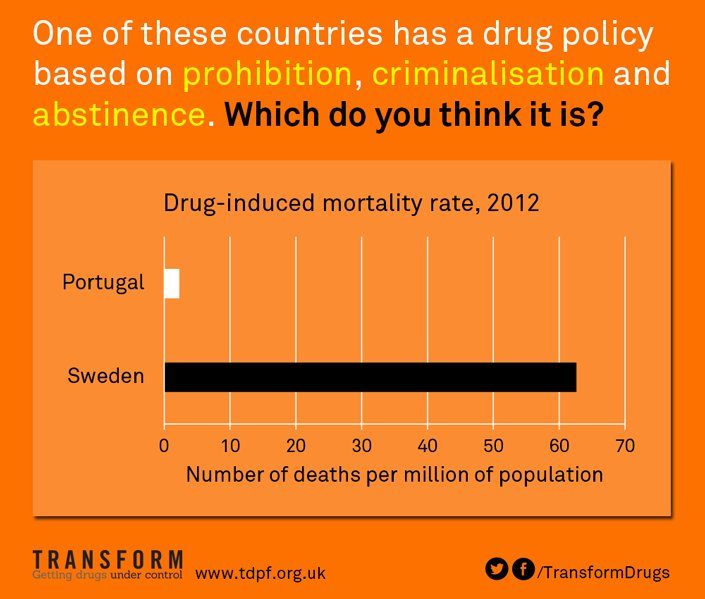
Further demonstrating that low levels of drug use do not necessarily equal low levels of drug-related harm, Sweden’s drug-induced mortality rate was 62.6 deaths per million in 2012, more than three times the European average of 17.1 deaths per million.21 In 2012, the drug-induced mortality rate in Portugal – which complemented its decriminalisation policy with an expansion of harm reduction services – was just 2.3 deaths per million.22 Sweden’s is therefore 30 times higher.
Some progress has been made, however, as Sweden’s rate of overdose deaths has led some to recognise that a new approach is required. OST and NSP provision is certainly better than it was ten years ago, but is still not nearly enough. Political bureaucracy and the continued use of drug-free rhetoric remain a barrier to the comprehensive programmes needed, and have meant Sweden has been unwilling to support such programmes on the international stage.
Sweden’s pursuit of a punitive, abstinence-based approach to drugs, coming at the expense of proven harm reduction services, has had negative consequences for the health and wellbeing of its drug-using population. These consequences would most likely be even more severe were it not for the country’s comprehensive health and social welfare system, as well as its culture of temperance. Ultimately, the case of Sweden emphasises that prevalence of drug use is only one measure of success – overall health harms cannot be ignored.
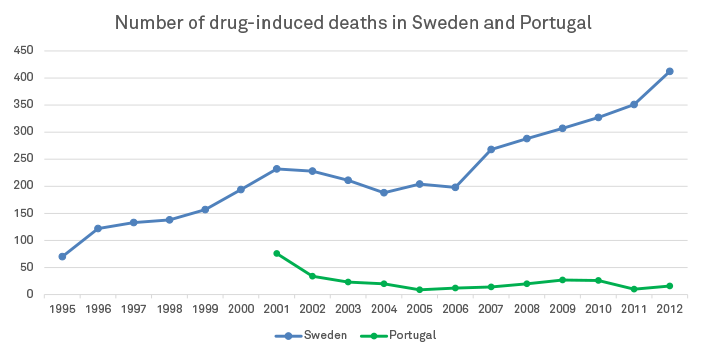
Comparing unadjusted figures like these would obviously be misleading if Sweden’s total population was significantly higher than Portugal’s. However, the two countries have similar population sizes, with Portugal’s (10.5 million) in fact slightly higher than Sweden’s (9.5 million)
References
- Tham, H. (2009) ‘The issue of criminalization of drug use in Sweden’, Nordic Studies on Alcohol and Drugs, vol. 26, pp. 432-435. http://www.nordicwelfare.org/PageFiles/4758/HenrikTham.pdf
- Johansson, P. and DuPont, R. L. (2009) ‘Drug policy choices – the Swedish way’. http://www.ibhinc.org/pdfs/DrugPolicyChoicesTheSwedishWayClean.pdf
- Swedish National Institute of Public Health (2013) ‘2013 National Report (2012 data) to the EMCDDA by the Reitox National Focal Point’., p. 83. http://www.folkhalsomyndigheten.se/pagefiles/12993/A2013-02-National-Report-2013-to-the-EMCDDA.pdf
- United Nations Office on Drugs and Crime (2007) ‘Sweden’s successful drug policy: a review of the evidence’. https://www.unodc.org/pdf/research/Swedish_drug_control.pdf
- Sweden is the joint second-largest funder of the UNODC (at 13.5%, with Germany), behind Japan at 19% but ahead of the US (13%).
- United Nations Office on Drugs and Crime (2006) ‘UN drugs chief praises Swedish drug control model’. http://www.unodc.org/unodc/en/press/releases/press_release_2006-09-06.html
- Degenhardt L. et al. (2008) ‘Toward a Global View of Alcohol, Tobacco, Cannabis, and Cocaine Use: Findings from the WHO World Mental Health Surveys’, PLoS Medicine. www.plosmedicine.org/article/info%3Adoi%2F10.1371%2Fjournal.pmed.0050141
- UK Home Office (2014) ‘Drugs: International Comparators’. https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/368489/DrugsInternationalComparators.pdf
- Tham, H. (2009) op. cit.
- European School Survey Project on Alcohol and Other Drugs (2011) ‘The 2011 ESPAD Report Substance Use Among Students in 36 European Countries’, p. 357. http://www.can.se/contentassets/8d8cb78bbd28493b9030c65c598e3301/the_2011_espad_report_full.pdf
- Ibid., p. 360.
- Ibid., p. 362.
- Balsa, C., et al. (2013) op. cit., p. 52.
- European Monitoring Centre for Drugs and Drug Addiction (2014) ‘Data and statistics’. http://www.emcdda.europa.eu/data/2014
- European School Survey Project on Alcohol and Other Drugs (2011) op. cit., p. 119.
- Skretting, A. and Rosenqvist, S. (2010) ‘Shifting focus in substitution treatment in the Nordic countries’, Nordic Studies on Alcohol and Drugs, vol. 27, pp. 581-598.
- Statens Offentliga Utredningar (2011) ‘Bättre insatser vid missbruk och beroende: Individen, kunskapen och ansvaret’. http://www.regeringen.se/content/1/c6/16/71/05/4a710efb.pdf
- Harm Reduction International (2012) ‘The Global State of Harm Reduction: Towards an Integrated Response’. http://www.ihra.net/files/2012/07/24/GlobalState2012_Web.pdf
- European Monitoring Centre for Drugs and Drug Addiction (2012) ‘Harm reduction overview for Sweden’. http://www.emcdda.europa.eu/country-data/harm-reduction/Sweden
- Karolinska Institutet (2013) ‘HIV/HCV Co-infection in Sweden – Epidemiology, HCV Treatment and the Importance of il28b Gene Polymorphism’. https://publications.ki.se/xmlui/bitstream/handle/10616/41788/Thesis_Jenny_Stenkvist.pdf?sequence=1
- European Monitoring Centre for Drugs and Drug Addiction (2014) ‘Country overview: Sweden – Drug-induced deaths and mortality among drug users’. http://www.emcdda.europa.eu/publications/country-overviews/se#drd
- Calculated based on the number of drug-induced deaths (16) in Portugal as a proportion of 15-64-year-olds in 2012. Source for number of deaths: European Monitoring Centre for Drugs and Drug Addiction (2014) ‘Data and statistics’. http://www.emcdda.europa.eu/data/2014


